SURGICAL ANATOMY by JOSEPH MACLISE
COMMENTARY ON PLATE 47.
THE SURGICAL DISSECTION OF THE PRINCIPAL BLOODVESSELS AND
NERVES OF THE ILIAC AND FEMORAL REGIONS.
Through the groin, as through the axilla, the principal blood vessels
and nerves are transmitted to, the corresponding limb. The main artery
of the lower limb frequently becomes the subject of a surgical
operation. The vessel is usually described as divisible into parts,
according to the regions which it traverses. But, as in examining any
one of those parts irrespective of the others, many facts of chief
surgical importance are thereby obscured and overlooked, I propose to
consider the vessel as a whole,
continuous from the aorta to where it
enters the popliteal space. The general course and position of the main
artery may be described as follows:--The abdominal aorta, A, bifurcates
on the body of the fourth lumbar vertebra. The level of the aortic
bifurcation corresponds with the situation of the navel in front, and
the crista ilii laterally. The aorta is in this situation borne so far
forwards by the lumbar spine as to occupy an almost central position in
the cavity of the abdomen. If the abdomen were pierced by two lines, one
extending from a little to the left side of the navel, horizontally
backwards to the fourth lumbar vertebra, and the other from immediately
over the middle of one crista ilii, transversely to a corresponding
point in the opposite side, these lines would intersect at the aortic
bifurcation. The two arteries, G G,* into which the aorta divides
symmetrically at the median line, diverge from one another in their
descent towards the two groins. As both vessels correspond in form and
relative position, the description of one will serve for the other.
While the thigh is abducted and rotated outwards, if a line be drawn
from the navel to a point, D, of the inguinal fold, midway between B,
the anterior iliac spine, and C, the symphysis pubis, and continued
thence to the inner condyle of the femur, it would indicate the general
course of the artery, G I W. In this course, the vessel may be regarded
as a main trunk, giving off at intervals large branches for the supply
of the pelvic organs, the abdominal parietes, and the thigh. From the
point where the vessel leaves the aorta, A, down to the inguinal fold,
D, it lies within the abdomen, and here, therefore, all operations
affecting the vessel are attended with more difficulty and danger than
elsewhere, in its course.
The artery of the lower limb, arising at the bifurcation of the aorta on
the fourth lumbar vertebra, descends obliquely outwards to the
sacra-iliac junction, and here it gives off its first branch, G,
(internal iliac,) to the pelvic organs. The main vessel is named common
iliac, at the interval between
its origin from the aorta and the point
where it gives off the internal iliac branch. This interval is very
variable as to its length, but it is stated to be usually two inches.
The artery, I, continuing to diverge in its first direction from its
fellow of the opposite side, descends along the margin of the true
pelvis as far as Poupart's ligament, D, where it gives off its next
principal branches,--viz., the epigastric and circumflex iliac. At the
interval between the internal iliac and epigastric branches, the main
artery, I, is named external iliac;
and the surgical length of this part
is also liable to vary, in consequence of the epigastric or circumflex
iliac branches arising higher up or lower down than usual. The main
vessel, after passing beneath the middle of Poupart's ligament, D, next
gives off the profundus branch, N, to supply the thigh. This branch
generally arises at a point an inch and half or two inches below the
fold of the groin; and between it and the epigastric above, the main
artery is named common femoral.
From the point where the profundus
branch arises, down to the popliteal space, the vessel remains as an
undivided trunk, being destined to supply the leg and foot. In this
course, the artery is accompanied by the vein, H K O, which, according
to the region in which it lies, assumes different names, corresponding
to those applied to the artery. Both vessels may now be viewed in
relation to each other, and to the several structures which lie in
connexion with them.
The two vessels above Poupart's ligament lie behind the intestines, and
are closely invested by the serous membrane. The origin of the vena
cava, F, lies close to the right side of the bifurcation of the aorta,
A; and here both vessels are supported by the lumbar spine. Each of the
two arteries, G G,* into which the aorta divides, has its accompanying
vein, H, on its inner side, but the common iliac part of the right
artery is seen to lie upon the upper portions of both the veins, as
these joining beneath it form the commencement of the vena cava. The
external iliac part, I, of each artery has its vein, K, on its inner
side. At the point, G, where the artery gives off its internal iliac
branch, the ureter, g,
crosses it, and thence descends to the bladder.
The internal iliac branch subdivides in general so soon after its
origin, that it may be regarded as for the most part an unsafe
proceeding to place a ligature upon it.
The iliac vessels, A G I, in approaching Poupart's ligament along the
border of the true pelvis, are supported by the psoas muscle, and
invested and bound to their place by the peritonaeum, and a thin process
of the iliac fascia. Some lymphatic glands are here found to lie over
the course of the vessels. The spermatic artery and vein, together with
the genito-crural nerve, descend along the outer border of the iliac
artery. When arrived at Poupart's ligament, the iliac vessels, I K,
become complicated by their own branches, and also by the spermatic
vessels, as these are about to pass from the abdomen through the
internal inguinal ring. While passing beneath the middle of Poupart's
ligament, D, the iliac artery, I, having its vein, K, close to its inner
side, rests upon the inner border of the psoas muscle, and in this place
it may be effectually compressed against the os pubis. The anterior
crural nerve, P, which in the iliac region lies concealed by the psoas
muscle, and separated by this from the vessels, now comes into view,
lying on the outer side of the artery. When the vessels have passed from
beneath Poupart's ligament, the serous membrane no longer covers them,
but the fibrous membrane is seen to invest them in the form of a sheath,
divided into two compartments, one of which (internal) receives the
vein, the other the artery. The iliac vessels, in passing to the thigh,
assume the name of femoral.
The femoral vessels, O N W, in the upper third of the thigh traverse a
triangular space, the base of which is formed by Poupart's ligament, D,
whilst the sides and apex are formed by the sartorius, Q, and adductor
longus muscles, T, approaching each other. In the undissected state of
the part, the structures which bound this space can in general be easily
recognised. A central depression extends from the middle of its base, D,
to its apex, V, and marks the course of the vessels. Near the middle of
Poupart's ligament, the vessels are comparatively superficial, and here
the artery may be felt pulsating; but lower down, as they approach the
apex of the triangle, the vessels become gradually deeper, till the
sartorius muscle inclining from its origin obliquely inwards to the
centre of the thigh, w, at length overlaps them. The inner border of the
sartorius muscle at the lower part of the upper third of the thigh, W,
guides to the position of the artery. Whilst traversing the femoral
triangle, the vessels enclosed in their proper sheath are covered by the
fascia lata, adipose membrane, and integument. In this place they lie
imbedded in loose cellular and adipose tissue. The femoral vein, O, is
on the same plane with the artery near Poupart's ligament; but from this
place downwards through the thigh, the vein gradually winds from the
inner to the back part of the artery; and when both vessels pass under
cover of the sartorius, they enter a strong fibrous sheath, V, derived
from the tendons of the adductor muscles upon which they lie. The artery
approaches the shaft of the femur near its middle; and in this place it
may be readily compressed against the bone by the hand. The anterior
crural nerve, P, dividing on the outer side of the artery, sends some of
its branches coursing over the femoral sheath; and one of these--the
long saphenous nerve--enters the sheath and follows the artery as far as
the opening in the great adductor tendon. The femoral artery, before it
passes through this opening into the popliteal space, gives off its
anastomatic branch. The profundus branch, N, springs from the outer side
of the femoral artery usually at a distance of from one to two inches
(seldom more) below Poupart's ligament, and soon subdivides. [Footnote]
The femoral artery in a few instances has been found double.
[Footnote: The ordinary length of each part of the main artery is stated
on the authority of Mr. Quain. See "Anatomy of the Arteries," &c. ]
The main artery of the lower limb may be exposed and tied in any part of
its course from the aorta to the popliteal space. But the situation most
eligible for performing such an operation depends of course upon
circumstances, both anatomical and pathological. If an aneurism affect
the popliteal part of the vessel, or if, from whatever cause arising, it
be found expedient to tie the femoral above this part, the place best
suited for the operation is that where the artery, W, first passes under
cover of the sartorius muscle. [Footnote] For, considering that
the
vessel gives off no important branch destined to supply any part of the
thigh or leg between the profundus branch and those into which it
divides below the popliteal space, the arrest to circulation will be the
same in amount at whichever part of the vessel between these two points
the ligature be applied. But since the vessel in the situation specified
can be reached with greater facility here than elsewhere lower down; and
since, moreover, a ligature applied to it here will be sufficiently
removed from the profundus branch above, and the seat of disease below,
to produce the desired result, the choice of the operator is determined
accordingly. The steps of the operation performed at the situation W,
where the artery is about to pass beneath the sartorius, are these: an
incision of sufficient length--from two to three inches--is to be made
over the course of the vessel, so as to divide the skin and adipose
membrane, and expose the fascia lata, through which the inner edge of
the sartorius muscle becomes now readily discernible. A vein (anterior
saphena) may be found to cross in this situation, but the saphena vein
proper is not met with, as this lies nearer the inner side of the thigh.
The fascia having been next divided, the edge of the sartorius is to be
turned aside, and now the pulsation of the artery in its sheath will
indicate its exact position. The sheath is next to be opened, for an
extent sufficient only to carry the point of the ligature-needle safely
around the artery, care being taken not to injure the femoral vein,
which lies close behind it, and also to exclude any nerve which may lie
in contact with the vessel.
[Footnote: This is the situation chosen by Scarpa for arresting by
ligature the circulation through the femoral artery in cases of
popliteal aneurism. The reasons stated in the text are those which
determine the surgeon to perform the operation in this place in
preference to that (the lower third of the thigh) where Mr. Hunter first
proposed to tie the vessel.]
If an aneurism affect the common femoral portion of the artery, the
external iliac part would require to be tied, because, between the seat
of the tumour and the epigastric and circumflex ilii branches above,
there would not be sufficient space to allow the ligature to rest
undisturbed; and even if the aneurism arose from the femoral below the
profundus branch in the upper third of the thigh, or if, after
amputation of the thigh, a secondary haemorrhage took place from the
femoral and the profunda arteries, a ligature would with more safety be
applied to the external iliac part than to the common femoral; because
of this latter, even when of its clear normal length, presenting so
small an interval between the epigastric and profundus branches. In
addition to this, it must be noticed, that occasionally the
profundus
itself, or some one of its branches, (external and internal circumflex,
&c.), arises as high up as Poupart's ligament, close to the origin
of
the epigastric and circumflex iliac. [Footnote]
[Footnote: The main artery (Plate 47) has been exposed in the iliac and
femoral regions with the object of showing the relation which its parts
bear to each other and to the whole; all the other dissections have been
made upon the same plan, the practical tendency of which will be
illustrated when considering the subject of arterial anastomosis.]
The external iliac part of the artery, G I, when requiring to be tied,
may be reached in the following way: an incision, commencing above the
anterior iliac spine, B, is to be carried inwards parallel to, and
above, Poupart's ligament, D, as far as the outer margin of the internal
abdominal ring. This incision is the one best calculated for avoiding
the epigastric artery, and for not disturbing the peritonaeum more than
is necessary. The skin and the three abdominal muscles having been
successively incised, the fibrous transversalis fascia is next to be
carefully divided, so as to expose the peritonaeum. This membrane is
then to be gently raised by the fingers, from off the iliacus and psoas
muscles as far inwards as the margin of the true pelvis where the artery
lies. On raising the peritonaeum the spermatic vessels will be found
adhering to it. The iliac artery itself is liable to be displaced by
adhering to the serous membrane, when this is being detached from the
inner side of the psoas muscle. [Footnote] The artery having been
divested of its serous covering as far up as a point midway between I G,
the epigastric and internal iliac branches, the ligature is to be passed
around it in this place, as being equidistant from these two sources of
disturbance. As the vein, K, lies close along the inner side of the
artery, the point of the instrument should first be inserted between
them, and passed from within outwards, in order to avoid wounding the
vein. If an aneurism affect the upper end of the external iliac artery,
it is proposed to tie the common iliac; but this is an operation of so
serious a nature, that it can in this respect be exceeded only by tying
the aorta itself. The common iliac artery is so situated, that it can as
easily be reached from the groin upwards as from the side of the abdomen
inwards, and in both directions the peritonaeum would have to be
disturbed to an equal extent.
[Footnote: The student, in operating upon the dead subject, is often
puzzled to find that the iliac artery does not appear in its usual
situation, unaware at the time that he has lifted the vessel in
connexion with the peritonaeum. I have once seen a very distinguished
surgeon, whilst performing this operation on the living body, at fault
owing to the same cause.]
DESCRIPTION OF PLATE 47.
A. The aorta at its point of bifurcation.
B. The anterior superior iliac spine.
C. The symphysis pubis.
D. Poupart's ligament, immediately above which are seen the circumflex
ilii and epigastric arteries, with the vas deferens and
spermatic
vessels.
E E*. The right and left iliac muscles covered by the peritonaeum; the
external cutaneous nerve is seen through
the membrane.
F. The vena cava.
G G*. The common iliac arteries giving off the internal iliac branches
on the sacro-iliac symphyses; g g, the
right and left ureters.
H H*. The right and left common iliac veins.
I I*. The right and left external iliac arteries, each is crossed by the
circumflex ilii vein.
K K *. The right and left external iliac veins.
L. The urinary bladder covered by the peritonaeum.
M. The rectum intestinum.
N. The profundus branch of the femoral artery.
O. The femoral vein; O, the
saphena vein.
P. The anterior crural nerve.
Q. The sartorius muscle, cut.
S. The pectinaeus muscle.
T. The adductor longus muscle.
U. The gracilis muscle.
V. The tendinous sheath given off from the long adductor muscle,
crossing the vessels, and becoming adherent to the vastus internus
muscle.
W. The femoral artery. The letter is on the part where the vessel
becomes first covered by the sartorius muscle.
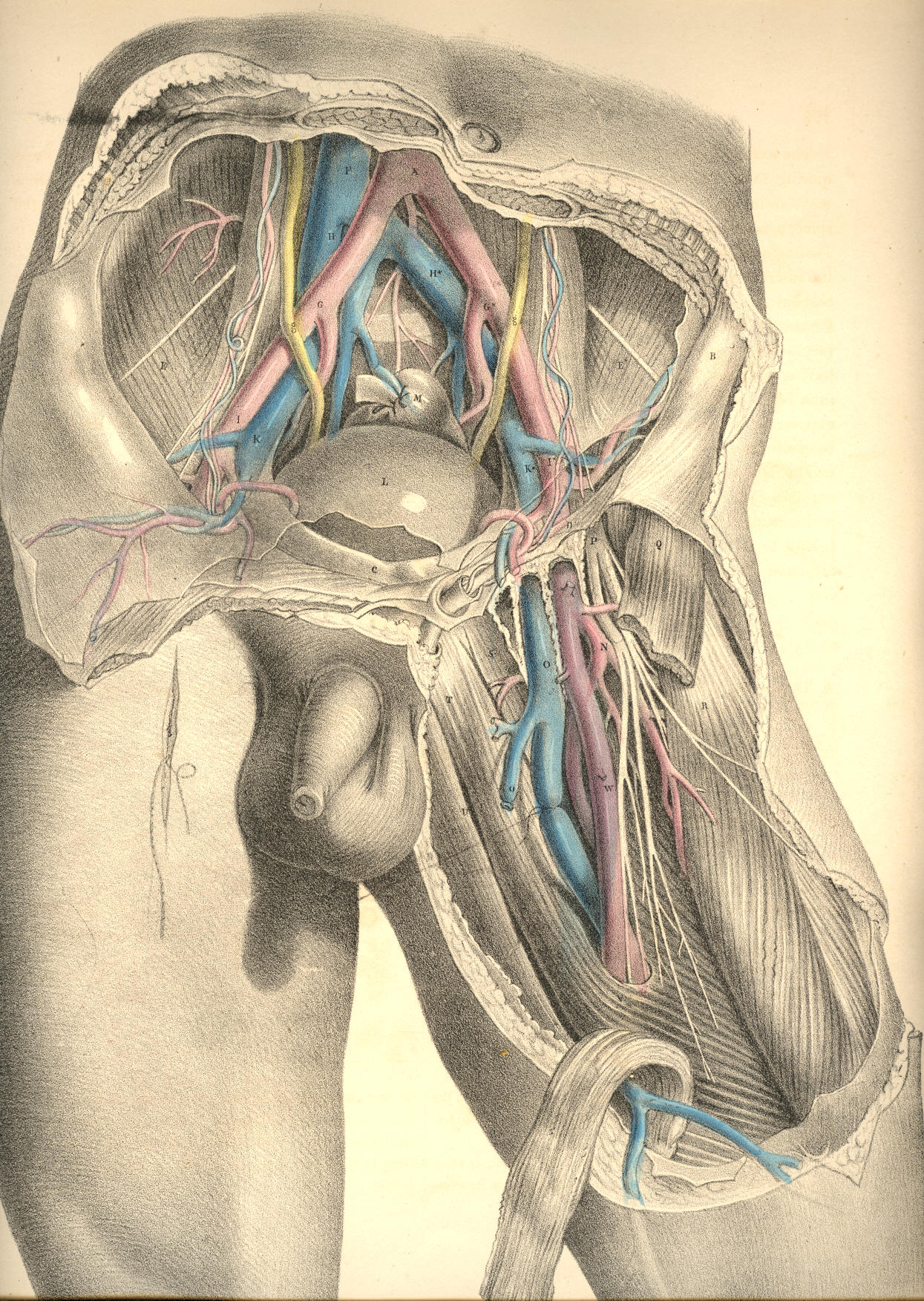
Plate 47.
COMMENTARY ON PLATES 48
& 49